Modes of mechanical ventilation refer to the various mechanical ventilator strategies employed to deliver a breath in patients that require mechanical ventilation1. The mode refers to the method of respiratory support. In general, mode selection is based on clinician familiarity and institutional preferences, since there is a paucity of evidence indicating that the mode affects clinical outcome. The most frequently used forms of volume-limited mechanical ventilation are intermittent mandatory ventilation (IMV) and continuous mandatory ventilation (CMV).2
Terminology
There has been extensive discussion regarding the nomenclature of mechanical ventilation, particularly in relation to the classification and terminology of ventilation modes. Despite these efforts, considerable confusion persists in the field. Ongoing initiatives aim to standardize and clarify this terminology, and, more recently, the International Organization for Standardization has revised its relevant standards to incorporate more precise definitions for modes of ventilation.3
Taxonomy for mechanical ventilation
The taxonomy is a logical classification system based on 10 maxims of ventilator design:4
10 maxims
How modes are classified
- A structured method is commonly used to classify modes of mechanical ventilation based on three key attributes: the control variable, the breath sequence, and the targeting scheme.
The control variable is the parameter directly regulated during inspiration. It is classified as pressure when inspiration is initiated with a preset inspiratory pressure or when pressure varies in proportion to inspiratory effort. It is classified as volume when both tidal volume and inspiratory flow are preset. If neither condition applies, the control variable is categorized as time.
The breath sequence is determined by analyzing whether breath initiation (triggering) and termination (cycling) are controlled by the patient or the ventilator. Based on these characteristics, breaths may be classified as mandatory or spontaneous and organized into sequences such as continuous mandatory ventilation (CMV) or intermittent mandatory ventilation (IMV).
The targeting scheme describes how the ventilator achieves the desired breath parameters. This may involve fixed operator-defined settings (set-point targeting) or dynamic adjustments made by the ventilator to achieve a specified goal (adaptive targeting), among other approaches.
Examples of mode classification
Assist/Control Volume Control (e.g., Covidien PB 840)
In this mode, inspiratory volume and flow are preset, establishing volume as the control variable. Each breath is volume-cycled, meaning that inspiration is terminated by the ventilator; such breaths are therefore classified as mandatory. Because all breaths are mandatory, the breath sequence is continuous mandatory ventilation (CMV). The operator directly sets the waveform parameters, indicating a set-point targeting scheme. Accordingly, the mode may be classified as volume-controlled continuous mandatory ventilation with set-point targeting (VC-CMV).
SIMV Volume Control Plus (e.g., Covidien PB 840)
In this mode, the operator sets the tidal volume but not the inspiratory flow. Since specifying volume alone is insufficient to define volume control, the control variable is classified as pressure. The presence of spontaneous breaths between mandatory breaths defines the breath sequence as intermittent mandatory ventilation (IMV). The ventilator adjusts inspiratory pressure between breaths to achieve a target average tidal volume, reflecting an adaptive targeting scheme. This mode may therefore be classified as pressure-controlled intermittent mandatory ventilation with adaptive targeting (PC-IMV, adaptive).
Descriptions of common modes
Mechanical ventilation machines are available with both invasive modes (such as intubation) and non-invasive modes (such as BPAP). Invasive has to do with the insertion of medical devices or tubes internal to the patient, while non-invasive is completely external to the patient, as for example in using a tightly fitting mask or other device that covers the patient's nose and mouth.
Assist mode, control mode, and assist-control mode
A basic distinction in mechanical ventilation is whether each breath is initiated by the patient (assist mode) or by the machine (control mode). Dynamic hybrids of the two (assist-control modes) are also possible, and control mode without assist is now mostly obsolete.
Airway pressure release ventilation
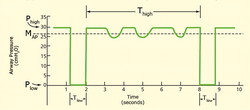
Airway pressure release ventilation is a time-cycled alternant between two levels of positive airway pressure, with the main time on the high level and a brief expiratory release to facilitate ventilation.567
Airway pressure release ventilation is a very versatile mode of ventilation. Like other modes, it needs to be well understood to use it effectively.8 The exhalation time (Tlow) is shortened to usually less than one second to maintain alveoli inflation. In the basic sense, this is a continuous pressure with a brief release.
Different perceptions of this mode may exist around the globe. While 'APRV' is common to users in North America, a very similar mode, biphasic positive airway pressure (BIPAP), was introduced in Europe.9 The term APRV has also been used in American journals where, from the ventilation characteristics, BIPAP would have been perfectly good terminology.10 But BiPAP is a trademark for a noninvasive ventilation mode in a specific ventilator (Respironics Inc.).
Other manufacturers have followed with their own brand names (BILEVEL, DUOPAP, BIVENT). Although similar in modality, these terms describe how a mode is intended to inflate the lung, rather than defining the characteristics of synchronization or the way spontaneous breathing efforts are supported.
Intermittent mandatory ventilation has not always had the synchronized feature, so the division of modes were understood to be SIMV (synchronized) vs IMV (not-synchronized). Since the American Association for Respiratory Care established a nomenclature of mechanical ventilation the "synchronized" part of the title has been dropped and now there is only IMV.
Mandatory minute ventilation
Mandatory minute ventilation (MMV) allows spontaneous breathing with automatic adjustments of mandatory ventilation to the meet the patient's preset minimum minute volume requirement. If the patient maintains the minute volume settings for VT x f, no mandatory breaths are delivered.
If the patient's minute volume is insufficient, mandatory delivery of the preset tidal volume will occur until the minute volume is achieved. The method for monitoring whether or not the patient is meeting the required minute ventilation (VE) differs by ventilator brand and model, but, in general, there is a window of monitored time, and a smaller window checked against the larger window (i.e., in the Dräger Evita® line of mechanical ventilators there is a moving 20-second window, and every 7 seconds the current tidal volume and rate are measured) to decide whether a mechanical breath is needed to maintain the minute ventilation.
MMV is an optimal mode for weaning in neonatal and pediatric populations and has been shown to reduce long-term complications related to mechanical ventilation.11
Pressure-regulated volume control
Pressure-regulated volume control is an Assist Controlled Ventilation (ACV) based mode. Pressure-regulated volume control utilizes pressure-limited, volume-targeted, time-cycled breaths that can be either ventilator- or patient-initiated.
The peak inspiratory pressure delivered by the ventilator is varied on a breath-to-breath basis to achieve a target tidal volume that is set by the clinician.
For example, if a target tidal volume of 500 mL is set but the ventilator delivers 600 mL, the next breath will be delivered with a lower inspiratory pressure to achieve a lower tidal volume. Though PRVC is regarded as a hybrid mode because of its tidal-volume (VC) settings and pressure-limiting (PC) settings fundamentally PRVC is a pressure-control mode with adaptive targeting.
Continuous positive airway pressure
Continuous positive airway pressure (CPAP) is a non-invasive positive pressure mode of respiratory support. CPAP is a continuous pressure applied to keep the alveoli open and not fully deflate. This mechanism for maintaining inflated alveoli helps increase partial pressure of oxygen in arterial blood, an appropriate increase in CPAP increases the PaO2.
Automatic positive airway pressure
Automatic positive airway pressure (APAP) is a form of CPAP that automatically tunes the amount of pressure delivered to the patient to the minimum required to maintain an unobstructed airway on a breath-by-breath basis by measuring the resistance in the patient's breathing.
Bilevel positive airway pressure
Bilevel positive airway pressure (BPAP) is a mode used during non-invasive ventilation (NIV). First used in 1988 by Professor Benzer in Austria,12 it delivers a preset inspiratory positive airway pressure (IPAP) and expiratory positive airway pressure (EPAP). BPAP can be described as a Continuous Positive Airway Pressure system with a time-cycle change of the applied CPAP level.13
CPAP/APAP, BPAP, and other non-invasive ventilation modes have been shown to be effective management tools for chronic obstructive pulmonary disease, acute respiratory failure, sleep apnea, etc.14
Often BPAP is incorrectly referred to as "BiPAP". BiPAP is the name of a portable ventilator manufactured by Respironics Corporation; it is just one of many ventilators that can deliver BPAP.
Medical uses
BPAP has been shown to be useful in reducing mortality and reducing the need for endotracheal intubation when used in people with chronic obstructive pulmonary disease (COPD).15
High-frequency ventilation (Active)
The term active refers to the ventilator's forced expiratory system. In a HFV-A scenario, the ventilator uses pressure to apply an inspiratory breath and then applies an opposite pressure to force an expiratory breath. In high-frequency oscillatory ventilation (sometimes abbreviated HFOV) the oscillation bellows and piston force positive pressure in and apply negative pressure to force an expiration.16
High-frequency ventilation (Passive)
The term passive refers to the ventilator's non-forced expiratory system. In a HFV-P scenario, the ventilator uses pressure to apply an inspiratory breath and then returns to atmospheric pressure to allow for a passive expiration.
This is seen in High-Frequency Jet Ventilation, sometimes abbreviated HFJV. Also categorized under High Frequency Ventilation is High Frequency Percussive Ventilation, sometimes abbreviated HFPV. With HFPV it utilizes an open circuit to deliver its subtidal volumes by way of the patient interface known as the Phasitron.
Volume guarantee
Volume guarantee an additional parameter available in many types of ventilators that allows the ventilator to change its inspiratory pressure setting to achieve a minimum tidal volume. This is utilized most often in neonatal patients who need a pressure controlled mode with a consideration for volume control to minimize volutrauma.
Spontaneous breathing and support settings
Positive end-expiratory pressure
Positive end expiratory pressure (PEEP) is pressure applied upon expiration. PEEP is applied using either a valve that is connected to the expiratory port and set manually or a valve managed internally by a mechanical ventilator.
PEEP is a pressure that an exhalation has to bypass, in effect causing alveoli to remain open and not fully deflate. This mechanism for maintaining inflated alveoli helps increase partial pressure of oxygen in arterial blood, and an increase in PEEP increases the PaO2.17
Pressure support
Pressure support is a spontaneous mode of ventilation also named Pressure Support Ventilation (PSV). The patient initiates every breath and the ventilator delivers support with the preset pressure value. With support from the ventilator, the patient also regulates their own respiratory rate and their tidal volume.
In Pressure Support, the set inspiratory pressure support level is kept constant and there is a decelerating flow. The patient triggers all breaths. If there is a change in the mechanical properties of the lung/thorax and patient effort, the delivered tidal volume will be affected. The user must then regulate the pressure support level to obtain desired ventilation.1819
Pressure support improves oxygenation,20 ventilation and decreases work of breathing.
Also see adaptive support ventilation.
Other ventilation modes and strategies
Flow-controlled ventilation
Flow-controlled ventilation (FCV) is an entirely dynamic ventilation mode, without pauses, with continuous and stable gas flows during both inspiration and expiration, aiming for linear changes in both volume and pressure.21 FCV is an invasive ventilation mode but, unlike Volume- and pressure controlled modes, it does not rely on a passive expiration created by collapse of the thoracic wall and elastic recoil of the lungs. A high resistant breathing circuit inhibits a passive expiration and therewith allows to fully control and stabilize the expiration flow. FCV creates an inspiration by generating a stable flow from a set End-expiratory pressure (EEP) to a set Peak pressure. Then a stable expiratory flow is created by suctioning.22 This expiratory flow rate is preferably similar to the inspiratory flow, aiming for an I:E ratio of 1:1.0, to minimize energy dissipation in the lungs.2324 FCV is a more efficient ventilation as compared to conventional modes,2526 allows ventilation through even small lumens (~2 – 10 mm ID)2728 and results in less applied mechanical power.25 FCV was invented by Professor Dr. med. Dietmar Enk.21
Negative pressure ventilation
Negative-pressure ventilation stimulates (or forces) breathing by periodic application of partial vacuum (air pressure reduced below ambient pressure), applied externally to the patient's torso—specifically, chest and abdomen—to assist (or force) the chest to expand, expanding the lungs, resulting in voluntary (or involuntary) inhalation through the patient's airway.293031
Various "negative pressure ventilators" (NPVs) have been developed to serve this function—most famously the "Iron lung," a tank in which the patient lays, with only their head exposed to ambient air, while air pressure on the remainder of their body, inside the tank, is varied by pumping, to stimulate chest and lung expansion and contraction. Though not in wide use today, NPVs were the principal forms of hospital and long-term mechanical ventilation in the first half of the 20th century, and remain in limited use today.293031
Closed loop systems
Adaptive Support Ventilation ASV and Adaptive Ventilation Mode AVM
These Modes uses employ optimal targeting323334 in which frequency and tidal volume of breaths of a patient on the ventilator are automatically adjusted and optimized to mimic natural breathing, stimulate spontaneous breathing, and reduce weaning time. In the ASV mode, every breath is synchronized with patient effort if such an effort exists, and otherwise, full mechanical ventilation is provided to the patient.3536
Automatic Tube Compensation
Automatic Tube Compensation (ATC) is the simplest example of a computer-controlled targeting system on a ventilator. It is a form of servo targeting37.
The goal of ATC is to support the resistive work of breathing through the artificial airway.
Neurally Adjusted Ventilatory Assist
Neurally Adjusted Ventilatory Assist (NAVA) is adjusted by a computer (servo) and is similar to ATC but with more complex requirements for implementation3839.
In terms of patient-ventilator synchrony, NAVA supports both resistive and elastic work of breathing in proportion to the patient's inspiratory effort
Proportional Assist Ventilation
Proportional assist ventilation (PAV) is another servo targeting based mode in which the ventilator guarantees the percentage of work regardless of changes in pulmonary compliance and resistance.40
The ventilator varies the tidal volume and pressure based on the patient's work of breathing. The amount it delivers is proportional to the percentage of assistance it is set to give.
PAV, like NAVA, supports both restrictive and elastic work of breathing in proportion to the patient's inspiratory effort.
Liquid ventilation
Liquid ventilation is a technique of mechanical ventilation in which the lungs are insufflated with an oxygenated perfluorochemical liquid rather than an oxygen-containing gas mixture. The use of perfluorochemicals, rather than nitrogen, as the inert carrier of oxygen and carbon dioxide offers a number of theoretical advantages for the treatment of acute lung injury, including:
- Reducing surface tension by maintaining a fluid interface with alveoli
- Opening of collapsed alveoli by hydraulic pressure with a lower risk of barotrauma
- Providing a reservoir in which oxygen and carbon dioxide can be exchanged with pulmonary capillary blood
- Functioning as a high-efficiency heat exchanger
Despite its theoretical advantages, efficacy studies have been disappointing and the optimal clinical use of LV has yet to be defined.41
Total liquid ventilation
In total liquid ventilation (TLV), the entire lung is filled with an oxygenated PFC liquid, and a liquid tidal volume of PFC is actively pumped into and out of the lungs. A specialized apparatus is required to deliver and remove the relatively dense, viscous PFC tidal volumes, and to extracorporeally oxygenate and remove carbon dioxide from the liquid.424344
Partial liquid ventilation
In partial liquid ventilation (PLV), the lungs are slowly filled with a volume of PFC equivalent or close to the FRC during gas ventilation. The PFC within the lungs is oxygenated and carbon dioxide is removed by means of gas breaths cycling in the lungs by a conventional gas ventilator.45
See also
See also
- Table of modes of mechanical ventilation
- Mechanical ventilation – Method to mechanically assist or replace spontaneous breathing
- Prone ventilation
- Respiratory therapist – Practitioner in cardio-pulmonary medicine
- Bubble CPAP – Noninvasive form of ventilation for newborns
References
References
- Cairo J (2024). Pilbeam's Mechanical Ventilation. Physiological and clinical applications. Elsevier St. Louis. p. 574. ISBN 978-0-323-87164-8.
- Esteban A, Anzueto A, Alía I, Gordo F, Apezteguía C, Pálizas F, et al. (May 2000). "How is mechanical ventilation employed in the intensive care unit? An international utilization review". American Journal of Respiratory and Critical Care Medicine. 161 (5): 1450–1458. doi:10.1164/ajrccm.161.5.9902018. PMID 10806138.
- "ISO 19223:2019". ISO. Retrieved 2025-09-04.
- Chatburn RL, El-Khatib M, Mireles-Cabodevila E (November 2014). "A taxonomy for mechanical ventilation: 10 fundamental maxims". Respiratory Care. 59 (11): 1747–1763. doi:10.4187/respcare.03057. PMID 25118309.
- Stock MC, Downs JB, Frolicher DA (April 1986). "Airway Pressure Release Ventilation (APRV): A New Ventilatory Support Mode During Acute Lung Injury (ALI)". Critical Care Medicine. 14 (4): 366. doi:10.1097/00003246-198604000-00111. ISSN 1530-0293.
- "» History of APRV". www.tcavnetwork.org. Archived from the original on 2025-01-17. Retrieved 2025-03-03.
- Henzler D (2011). "What on earth is APRV?". Critical Care. 15 (1). London, England: 115. doi:10.1186/cc9419. PMC 3222047. PMID 21345265.
- Andrews P, Shiber J, Madden M, Nieman GF, Camporota L, Habashi NM (2022-07-25). "Myths and Misconceptions of Airway Pressure Release Ventilation: Getting Past the Noise and on to the Signal". Frontiers in Physiology. 13 928562. doi:10.3389/fphys.2022.928562. PMC 9358044. PMID 35957991.
- Baum M, Benzer H, Putensen C, Koller W, Putz G (September 1989). "[Biphasic positive airway pressure (BIPAP)--a new form of augmented ventilation]". Der Anaesthesist. 38 (9): 452–458. PMID 2686487.
- Putensen C, Zech S, Wrigge H, Zinserling J, Stüber F, Von Spiegel T, et al. (July 2001). "Long-term effects of spontaneous breathing during ventilatory support in patients with acute lung injury". American Journal of Respiratory and Critical Care Medicine. 164 (1): 43–49. doi:10.1164/ajrccm.164.1.2001078. PMID 11435237.
- Guthrie SO, Lynn C, Lafleur BJ, Donn SM, Walsh WF (October 2005). "A crossover analysis of mandatory minute ventilation compared to synchronized intermittent mandatory ventilation in neonates". Journal of Perinatology. 25 (10): 643–646. doi:10.1038/sj.jp.7211371. PMID 16079905.
- Benzer H (1988) Ventilatory support by intermittent changes in PEEP levels. 4th European Congress on Intensive Care Medicine. Baveno-Stresa
- Hörmann C, Baum M, Putensen C, Mutz NJ, Benzer H (January 1994). "Biphasic positive airway pressure (BIPAP)--a new mode of ventilatory support". European Journal of Anaesthesiology. 11 (1): 37–42. PMID 8143712.
- Levitt MA (November 2001). "A prospective, randomized trial of BiPAP in severe acute congestive heart failure". The Journal of Emergency Medicine. 21 (4): 363–369. doi:10.1016/s0736-4679(01)00385-7. PMID 11728761.
- Osadnik CR, Tee VS, Carson-Chahhoud KV, Picot J, Wedzicha JA, Smith BJ (July 2017). "Non-invasive ventilation for the management of acute hypercapnic respiratory failure due to exacerbation of chronic obstructive pulmonary disease". The Cochrane Database of Systematic Reviews. 2017 (7) CD004104. doi:10.1002/14651858.CD004104.pub4. hdl:10044/1/53458. PMC 6483555. PMID 28702957.
- Allardet-Servent J (December 2011). "High-frequency oscillatory ventilation in adult patients with acute respiratory distress syndrome: where do we stand and where should we go?". Critical Care Medicine. 39 (12): 2761–2762. doi:10.1097/CCM.0b013e31822a5c35. PMID 22094505.
- Schuster DP, Klain M, Snyder JV (October 1982). "Comparison of high frequency jet ventilation to conventional ventilation during severe acute respiratory failure in humans". Critical Care Medicine. 10 (10): 625–630. doi:10.1097/00003246-198210000-00001. PMID 6749433.
- "Servo-i Mechanical Ventilator". Getinge AB. Retrieved 17 May 2025.
- "Servo-s Mechanical Ventilator". Getinge AB. Retrieved 17 May 2025.
- Spieth PM, Carvalho AR, Güldner A, Kasper M, Schubert R, Carvalho NC, et al. (April 2011). "Pressure support improves oxygenation and lung protection compared to pressure-controlled ventilation and is further improved by random variation of pressure support". Critical Care Medicine. 39 (4): 746–755. doi:10.1097/CCM.0b013e318206bda6. PMID 21263322. S2CID 35876431.
- DE 102016109528A1, Enk D, "Verfahren und Vorrichtung zur Beatmung eines Patienten (method and device for ventilating a patient)", published 7 September 2017, assigned to Current Assignee Ventinova Technologies BV
- DE 102007013385A1, Enk D, "Gasstromumkehrelement (gas flow reversing element).", published 18 September
- Barnes T, van Asseldonk D, Enk D (December 2018). "Minimisation of dissipated energy in the airways during mechanical ventilation by using constant inspiratory and expiratory flows - Flow-controlled ventilation (FCV)". Medical Hypotheses. 121: 167–176. doi:10.1016/j.mehy.2018.09.038. PMID 30396474.
- Barnes T, Enk D (February 2019). "Ventilation for low dissipated energy achieved using flow control during both inspiration and expiration". Trends in Anaesthesia and Critical Care. 24: 5–12. doi:10.1016/j.tacc.2018.09.003.
- Weber J, Schmidt J, Straka L, Wirth S, Schumann S (April 2020). "Flow-controlled ventilation improves gas exchange in lung-healthy patients- a randomized interventional cross-over study". Acta Anaesthesiologica Scandinavica. 64 (4): 481–488. doi:10.1111/aas.13526. PMID 31828755.
- Sebrechts T, Morrison SG, Schepens T, Saldien V (February 2021). "Flow-controlled ventilation with the Evone ventilator and Tritube versus volume-controlled ventilation: A clinical cross-over pilot study describing oxygenation, ventilation and haemodynamic variables". European Journal of Anaesthesiology. 38 (2): 209–211. doi:10.1097/EJA.0000000000001326. PMID 33394805.
- Schmidt J, Günther F, Weber J, Kehm V, Pfeiffer J, Becker C, et al. (December 2019). "Glottic visibility for laryngeal surgery: Tritube vs. microlaryngeal tube: A randomised controlled trial". European Journal of Anaesthesiology. 36 (12): 963–971. doi:10.1097/EJA.0000000000001110. PMC 6855316. PMID 31644514.
- Meulemans J, Jans A, Vermeulen K, Vandommele J, Delaere P, Vander Poorten V (2020). "Evone® Flow-Controlled Ventilation During Upper Airway Surgery: A Clinical Feasibility Study and Safety Assessment". Frontiers in Surgery. 7 6. doi:10.3389/fsurg.2020.00006. PMC 7058692. PMID 32185179.
- Matioc AA (February 2018). "An Anesthesiologist's Perspective on the History of Basic Airway Management: The "Progressive" Era, 1904 to 1960". Anesthesiology. 128 (2): 254–271. doi:10.1097/ALN.0000000000001975. PMID 29112511.
Early Positive and Alternate Pressure Machines
- Rockoff, Mark, M.D., "The Iron Lung and Polio,", video (8 minutes), January 11, 2016, OPENPediatrics and Boston Children's Hospital on YouTube, retrieved April 11, 2020 (historical background and images, explanatory diagrams, and live demonstrations)
- Walkey A, Summer R (2008). "E. Noninvasive Mechanical Ventilation". Boston Medical Center ICU Manual (PDF). Boston University. p. 17.
Negative pressure
- Laubscher T, Heinrichs W, Weiler N, Hartmann G, Brunner J (1994). "An adaptive lung ventilation controller". IEEE Transactions on Biomedical Engineering. 41 (1): 51–59. doi:10.1109/10.277271.
- Tehrani FT (October 1991). "Automatic Control of an Artificial Respirator". Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society. Vol. 13. pp. 1738–1739. doi:10.1109/IEMBS.1991.684729. ISBN 978-0-7803-0216-7. S2CID 63221714.
- Chatburn RL, Mireles-Cabodevila E (January 2011). "Closed-loop control of mechanical ventilation: description and classification of targeting schemes". Respiratory Care. 56 (1): 85–102. doi:10.4187/respcare.00967. PMID 21235841.
- Tehrani FT (December 2008). "Automatic control of mechanical ventilation. Part 1: theory and history of the technology". Journal of Clinical Monitoring and Computing. 22 (6): 409–415. doi:10.1007/s10877-008-9150-z. PMID 19011976.
- Tehrani FT (December 2008). "Automatic control of mechanical ventilation. Part 2: the existing techniques and future trends". Journal of Clinical Monitoring and Computing. 22 (6): 417–424. doi:10.1007/s10877-008-9151-y. PMID 19020981.
- Fabry B, Guttmann J, Eberhard L, Wolff G (1994-05-01). "Automatic compensation of endotracheal tube resistance in spontaneously breathing patients". Technology and Health Care. 1 (4): 281–291. doi:10.3233/THC-1994-1405.
- Sinderby C (2002). "Neurally adjusted ventilatory assist (NAVA)". Minerva Anestesiol. 68 (5): 378–380.
- Beck J, Liu Y, Sinderby C (2016), "Noninvasive Neurally Adjusted Ventilatory Assist (NIV-NAVA) in Children and Adults", Noninvasive Mechanical Ventilation, Cham: Springer International Publishing, pp. 145–152, ISBN 978-3-319-21652-2, retrieved 2026-02-18
{{citation}}: CS1 maint: work parameter with ISBN (link) - Younes M (January 1992). "Proportional assist ventilation, a new approach to ventilatory support. Theory". The American Review of Respiratory Disease. 145 (1): 114–120. doi:10.1164/ajrccm/145.1.114. PMID 1731573.
- Degraeuwe PL, Vos GD, Blanco CE (October 1995). "Perfluorochemical liquid ventilation: from the animal laboratory to the intensive care unit". The International Journal of Artificial Organs. 18 (10): 674–683. doi:10.1177/039139889501801020. PMID 8647601. S2CID 13038566.
- Norris MK, Fuhrman BP, Leach CL (August 1994). "Liquid ventilation: it's not science fiction anymore". AACN Clinical Issues in Critical Care Nursing. 5 (3): 246–254. doi:10.4037/15597768-1994-3004. PMID 7780839.
- Greenspan JS (1996). "Physiology and clinical role of liquid ventilation therapy". Journal of Perinatology. 16 (2 Pt 2 Su): S47–S52. PMID 8732549.
- Dirkes S (June 1996). "Liquid ventilation: new frontiers in the treatment of ARDS". Critical Care Nurse. 16 (3): 53–58. doi:10.4037/ccn1996.16.3.53. PMID 8852261.
- Cox CA, Wolfson MR, Shaffer TH (April 1996). "Liquid ventilation: a comprehensive overview". Neonatal Network. 15 (3): 31–43. PMID 8715647.